I’ve surveyed over a thousand people on what they tried and what their health is now. Here are the key takeaways…
Many people recover and don’t know how it happened
Despite trying many treatments, many of the recovered report that nothing helped them or that time helped the most. They got better and they don’t know why. This is the most common way that people recover. You can recover without doing anything crazy or risky.
Maximizing your chances of recovery with data
I want to be responsible and do the right thing when I give out this information. So here’s the disclaimer:
While data exists on how you might maximize your chances, it may cause more harm than good.
Please understand that the data and The Science™ may turn out to be erroneous. Before there was Ozempic, Western doctors prescribed amphetamines for weight loss. ‘Medicine’ has a history of causing more harm than good.
Let’s get into the data, which may or may not be reliable.
HBOT (hyperbaric oxygen)
HBOT is the only treatment with a randomized controlled trial (RCT) that supports its use. A small fraction of patients saw a meaningful improvement. However, another RCT did NOT find a statistically significant difference. For more details, see this thread.
This is currently the most ‘proven’ treatment because it has the most credible RCT evidence supporting its use. See Long Haul Wiki for a list of all positive and negative RCTs on treatments.
Only ~5.8% of the people surveyed report trying high pressure HBOT. Recovery rates may be low because people don’t know about, aren’t trying, or aren’t getting access to the better treatments.
Almost everything has been tried
Before you get excited about a treatment that people are reporting success with, please know that thousands of patients means that less popular treatments have been tried by many people. I’ve made my survey data public so you can look up how many people tried a particular treatment (click this link).
![]() There is data on treatments that probably don’t work. You might as well avoid those.
There is data on treatments that probably don’t work. You might as well avoid those.
Out of everything that has been tried by 30+ people, the chances of recovery are very low.
![]() If you are hellbent on recovery, you should anticipate trying a lot of treatments.
If you are hellbent on recovery, you should anticipate trying a lot of treatments.
 There is no solid evidence that trying a lot of treatments is a good idea. The people who recover tend to try fewer treatments, though it may be a correlation rather than causation.
There is no solid evidence that trying a lot of treatments is a good idea. The people who recover tend to try fewer treatments, though it may be a correlation rather than causation.
![]() Time is a limited resource. Committing months or years to a single treatment means that you aren’t taking many shots on goal. (It’s probably a good idea to try treatments one at a time so that you will know what each individual treatment actually does.)
Time is a limited resource. Committing months or years to a single treatment means that you aren’t taking many shots on goal. (It’s probably a good idea to try treatments one at a time so that you will know what each individual treatment actually does.)
You can also look up how common negative experiences are. Some treatments that are supposed to be safe, e.g. acupuncture, don’t seem to actually be that safe ![]() . Exercise is the worst intervention when it comes to patients reporting negative experiences. A few treatments like pacing strategies and low histamine diet appear to be safe.
. Exercise is the worst intervention when it comes to patients reporting negative experiences. A few treatments like pacing strategies and low histamine diet appear to be safe.
Double edged swords
If there are treatments that help, survey data indicates that the majority of those treatments also cause negative experiences in some people. Perhaps one way around that is to:
- Start with low doses
- Stop treatment if symptoms are going in the wrong direction
This is the prudent approach commonly used for experimental medicine.
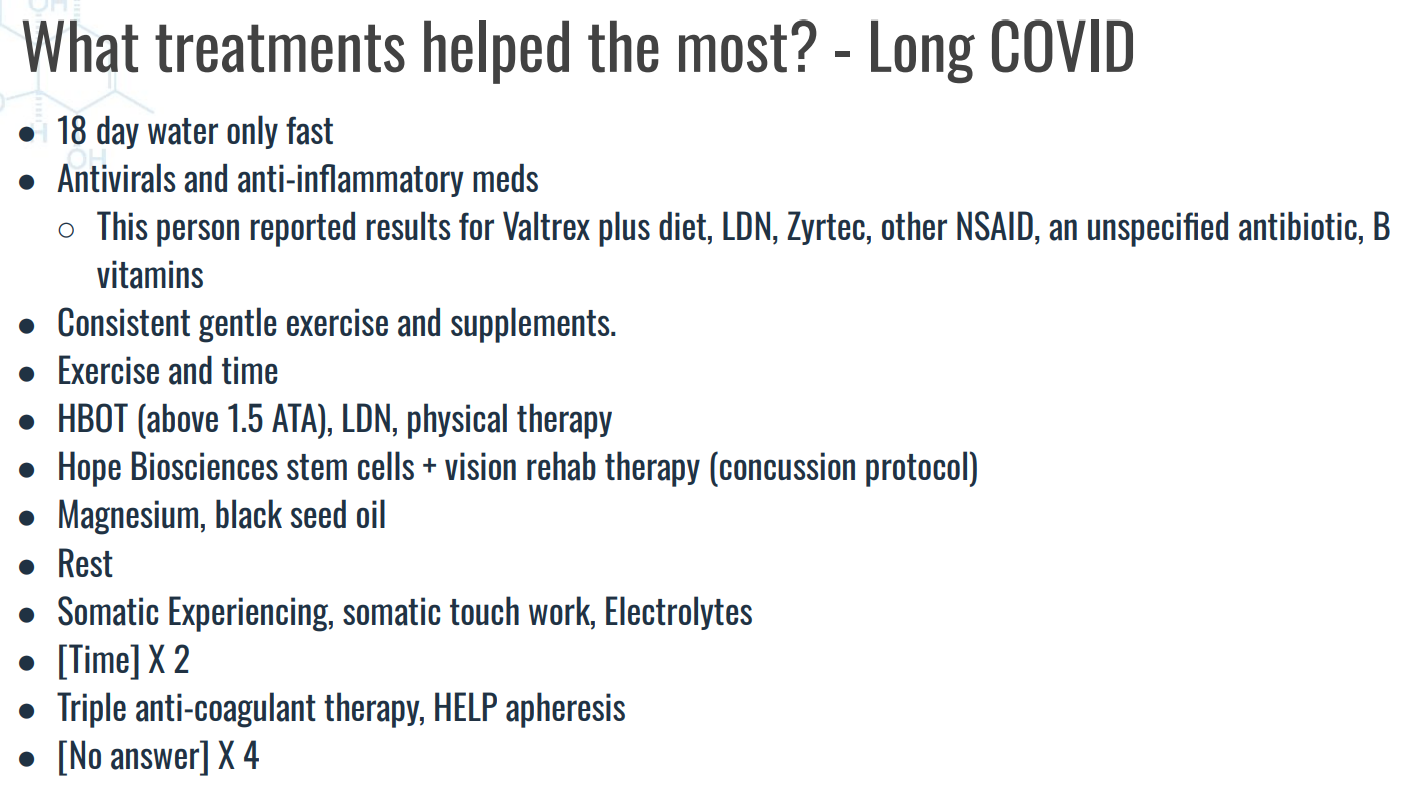
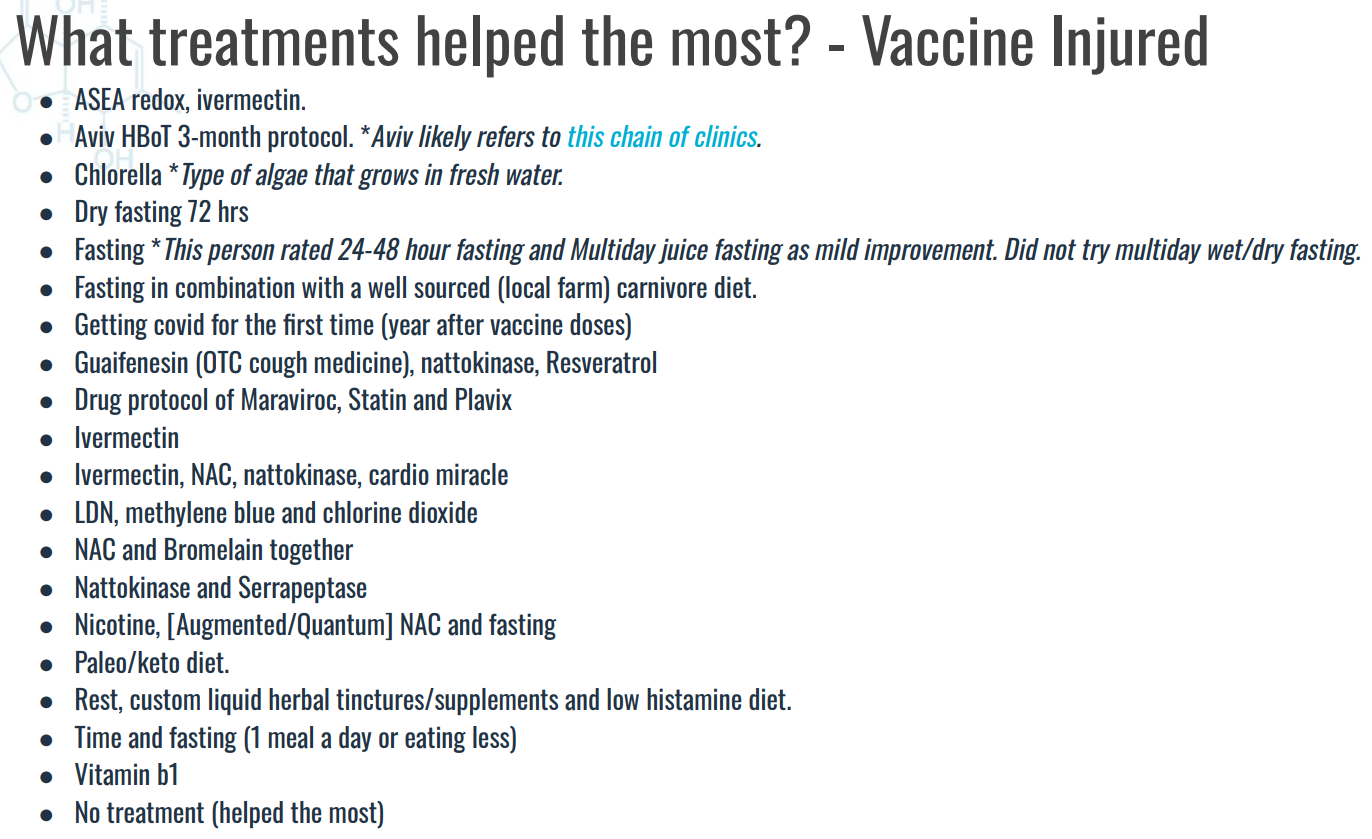
I’ve released the survey data on which treatments are the most likely to lead to recovery. When I have time I’ll make updated information more accessible (e.g. in an easy-to-understand list) like I did in this older video.
Why is long haul hard to treat?
Suppose that patients have already discovered the treatments that are effective. This would mean that there are multiple overlapping and inter-related causes for Long COVID, ME/CFS, and postvax (vaccine injury). Multiple underlying causes would explain why response rates for treatment are so low. It would also explain why symptoms are different from patient to patient- patients are drawing from the same pool of causes and symptoms but everybody gets a different combination.
We have no tests for determining the underlying causes. That means that we can’t predict the outcome of treatments… so the best that we can do is to try treatments one at a time.
Microbes as the cause of chronic illness would explain the underlying causes. Microbes would explain why (most) antimicrobials act as double edged swords. Antimicrobial treatments may be a good place to look for potential treatments.
- But, be very cautious with antibiotics. The risk/reward on them appears to be pretty bad; it would be prudent to avoid them.
And old list of antimicrobials can be found here (in the slides). Lion’s mane mushroom may be dangerous though, see r/LionsManeRecovery/ before proceeding.
What I would actually do myself
I’ve tried drugs from ex-Soviet bloc countries that aren’t approved in the West. I’m not a stranger to experimental medicine.
But now I realize that I shouldn’t have done anything crazy to recover. I should have stuck to eating a certain way and trying new foods (e.g. black seed oil). This is because different foods have different antimicrobial chemicals. People may be recovering because their diet changed over time. I explain that way of eating below:
Looking back, I would prioritize safety. Eating supermarket food is (likely) one of the safer things out there.
Recovery stories and compilations of recovery stories
You can find these in survey data, Reddit r/LongHaulersRecovery, and Youtube. There’s a decent summary of 60 stories from Reddit.
However, with time and experience, you will discover that there are various issues with these recovery stories.
Information is more unreliable than you think
Many of us are indoctrinated into thinking that the scientific literature is supposed to be credible because of peer review. However, I’ve compiled links to the scientific literature on Long COVID and postvax at Long Haul Wiki. You will quickly discover that the claimed results rarely line up with reality. And you may be disheartened to find that most doctors don’t know or don’t care about this.
We don’t have the answers that most patients want
I’ve really looked for answers.
- Highly experimental drugs that aren’t approved for human use anywhere (e.g. GS-44). Here’s how you figure out how to get them.
- Recovery stories
- The scientific literature
- Survey data that myself and others have collected
Patients have tried almost everything.
So the question is… have we already discovered the effective treatments? (There’s no solid evidence either way.)
- If the answer is no, then it’s a medical mystery as to why some people recover.
- If the answer is yes, then the recovery rates on those treatments are really low. You’ll likely need to try a lot of treatments.
A practical approach is to focus on risk and to try the treatments where the gamble (risk level) is acceptable to you. You get to decide the level of dumb / crazy / desperate that you are willing to accept.
So… that’s the best answer that we have right now. I wish we had better answers but it is what it is.