First of all, a ME/CFS patient seems to have committed suicide following HELP apheresis in Cyprus (details later on in this post). Whereas I would not describe HELP apheresis as a “safe” treatment, Beate Jaeger et al. do describe it as a safe treatment in their paper.
Secondly, the paper’s claim about 16/17 patients experiencing ‘a great benefit’ is questionable. We simply aren’t seeing such high response rates to any therapy.
Thirdly, very few people - somewhere around 7% - are seeing real recovery. They able to work again without accommodations and have minimal complaints about remaining symptoms. To be fair, most people use the word “recovery” to mean something else and set the bar very low. The Jaeger and colleagues paper claims “12 patients nearly reached full recovery”, which is an extraordinary claim.
The paper
Jaeger and her colleagues report results from the clinic in Germany:
We randomly assigned 17 Long COVID patients to receive repeated H.E.L.P. apheresis treatments in short intervals (1-7 sessions) until they recovered from major clinical symptoms. Of these 17 treated patients, 16 patients felt immediate improvement and 12 patients nearly reached full recovery after completion of the treatment. A 6–10-month follow-up revealed that 15 patients maintained their improvements. Thus, of the 17 patients with severe Long COVID symptoms, 16 patients had experienced a great benefit. One patient did not improve, although his oxygen saturation ameliorated. Therefore, H.E.L.P. apheresis serves as a promising and safe treatment option for Long COVID patients.
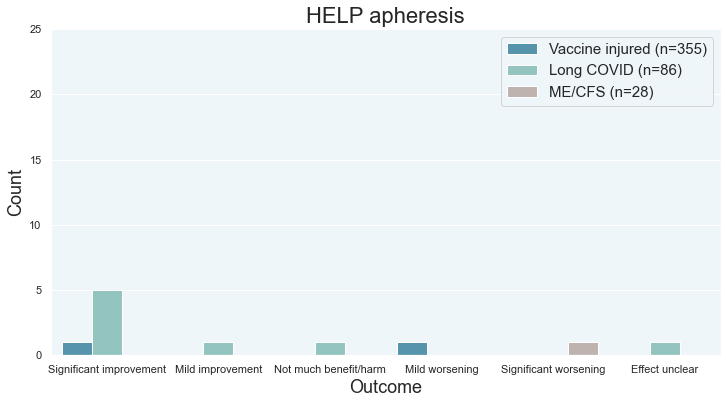
Survey data
I have limited data on 11 patients (not all of whom are Long COVID). 3 or 4 of those patients are non-responders.
Search for HELP apheresis here: Treatment Outcomes Survey analysis
Asad Khan
Khan is one of the co-authors on the Beate Jaeger and colleagues paper. He is a Long COVID sufferer and has undergone HELP apheresis himself.
In a June 13 2022 tweet, he described himself as “unwell” and unable to return to his former job as a doctor:
I cannot recommend or discourage any particular treatment. I am better than before but still unwell. I haven’t worked since Nov ‘20. Dr Jaeger saved my life but I do not have any official status in her clinic. I am a normal fee-paying patient there. 2/n
The ME/CFS patient who committed suicide
It is possible that HELP apheresis ultimately resulted in the death of a patient. A ME/CFS patient went to Cyprus, significantly deteriorated following treatment, and committed suicide some time later. This patient had previously worsened following COVID vaccination.
- Facebook post where Jack talks about his future plans to go to Cyprus
- Tweets about his passing.
- Facebook posts about his passing.
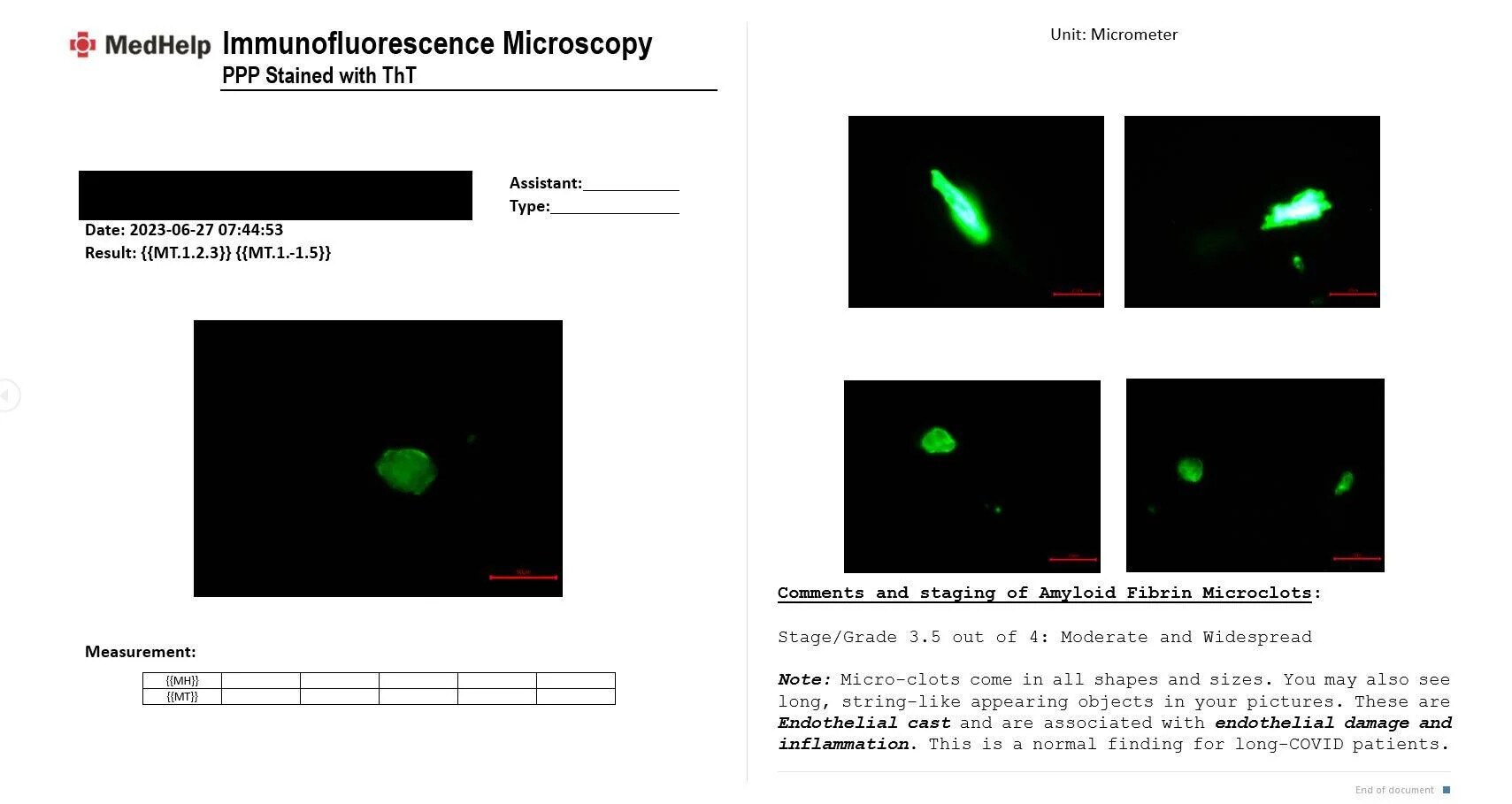
Microclot grading system
Pretorius, Kell, and others in their group have published numerous papers on microclots. The T2DM paper published Nov 2020 posted results from an objective system that measured amyloid area to determine the extent of microclotting.
Micrograph analysis was done using ImageJ (version 2.0.0-rc-34/1.5a). The % area of amyloid were calculated using the thresholding method. This method allows a measurement of area of amyloid signal.
Some subsequent papers used a grading system with both objective and subjective components. For example, version 1 of a pre-print described the grading system in Table 3 (Tables 2-4).
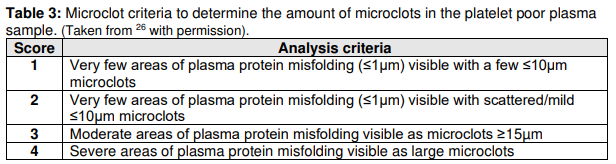
Some clinicians have switched to a grading system that is completely subjective. A potential issue with such a grading system is that there is a conflict of interest that would bia$ the results towards the patient needing treatment.
Oversight and accountability
The microclot researchers published version 1 of their pre-print claiming that all 24/24 patients were responders. Version 2 of that pre-print removed data on those 24 treatment patients. Nonetheless, the version 2 abstract calls for clinical trials without mentioning the previously-reported data:
Removal and reversal of these underlying endotheliopathies provide an important treatment option that urgently warrants controlled clinical studies to determine efficacy in patients with a diversity of comorbidities impacting on SARS-CoV-2 infection and COVID-19 severity.
It is strange for the researchers to call for RCTs while omitting their data that would be extremely relevant to their call to action.
We don’t have a reliable system to ensure that clinicians are accurately reporting patient outcomes. This is a major problem in the scientific literature right now as ‘everything works’. I’ve discussed that problem in the thread They can’t all be right - not everything works. Also see LongHaulWiki for a list of scientific papers where almost every treatment seems to be incredible.
Tracking adverse events
The Long COVID, ME/CFS, and vax injured chronic illness communities do not have a real system for tracking adverse events from experimental treatments. The “best” data available comes from anecdotes and anonymous reddit threads like this one on the Cyprus (not German) HELP apheresis clinic:
If you’re planning to do HELP apheresis, then please don’t go to the clinic in Larnaka, Cyprus.
The clinic tries very hard to silence people who speak up, and spreads misinformation about how great their clinic is, but the truth has to come out.
- Note: Beate Jaeger operates in Germany, not Cyprus. I do not believe that she is connected to the Cyprus clinic.
I believe that there is a MASSIVE problem with many chronic illness clinicians underrecognizing adverse events. It is the elephant in the room. We need to recognize that some people are responding very negatively to treatments that healthy people can handle- even for the supermarket food black seed oil. Once we recognize that, we can move forward and take steps to try to prevent unnecessary harm that is happening to patients. For example, we can start with low dosages and discontinue treatment that is going the wrong way.
The big picture
Patients desperately need clinicians to make a good faith effort to accurately track patient outcomes. Without it, there is a real risk that they will cause more harm than good. They cannot following the Hippocratic oath - “First do no harm” - if they don’t know if they’re causing harm in the first place.
Patients desperately need a functional healthcare system that serves their interests. To get there, we need to have honest, open discussions about the shortcomings of what we have now.