
Hydroxychloroquine (HCQ) has been used to treat lupus in humans for a long time (see DOI:10.1016/j.lpm.2014.03.007). It has also been tried for multiple sclerosis with mild success - patients with Primary progressive multiple sclerosis (PPMS) were less likely to worsen (DOI:10.1002/ana.26239). It is moderately useful for treating rheumatoid arthritis (DOI: https://doi.org/10.1002/acr.23826). Emerging evidence shows strong potential for use as a diabetes drug (DOI:10.1155/2020/5214751). Animal models of autoimmune disease suggest that it may be useful for other autoimmune diseases.
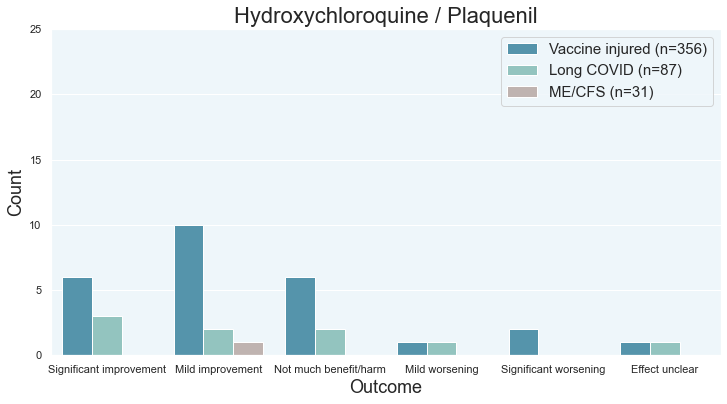
As far as chronic illness goes, one long hauler seemed to have recovered on it (data). Like with other long haul treatments, it may take 15-40+ people trying a treatment for somebody to recover from that treatment. HCQ was not very popular so the survey data is not that reliable.
Brief history
Chloroquine was used to treat the SARS1 virus and was one of the first experimental treatments for SARS2 as scientists had to improvise for a novel virus. Hydroxychloquine also saw use as it is similar to chloroquine but has better safety.
Then Donald Trump mentioned the drug. All sorts of politics happened and the drug earned a polarizing reputation (hence the tongue-in-cheek artwork at the beginning of this post). So the drug may have a certain stigma in certain circles. However, it is commonly used to treat and prevent malaria. Those travelling to Africa are often given hydroxychloroquine as a preventative measure.
Mechanisms of action
Anti-viral
Some people believe that it is effective against SARS2. Again, this is a controversial topic and some people believe that HCQ effectively does nothing against SARS2.
Anti-bacterial
It works against the Lyme bacteria (Borrelia). See Megan Weitner’s 2016 thesis or her lab’s publications that mentions hydroxychloroquine (e.g. this one). By itself, it’s not some sort of silver bullet against Lyme. However, its antimicrobal properties may explain why a few people get better.
Immunomodulatory
HCQ prevents the TLR7 protein from being split into two and ‘maturing’ into the version of the protein that does work. See DOI:10.1002/eji.202149361. The TLR7 protein is like a ‘security alarm’ that specifically looks for signs of pathogens that shouldn’t be there. In this case, TLR7 looks for single-stranded RNA (which is found in SARS1 and SARS2). In practice, there may be more benefit than harm when HCQ is used to prevent SARS2/COVID or to treat it early. See https://c19hcq.org/ for data. (I know HCQ for SARS2 can be a hugely controversial topic so let’s not get into it. There are a lot of people saying that the RCTs prove that it doesn’t work. It depends on which RCTs you believe.)
Weakening the TLR7 pathway affects how the body’s immune system works.
It is also believed to inhibit TLR9, the pathway that detects CpG (CpG islands are found in some pathogens). Torigoe and colleagues write:
[…] hydroxychloroquine markedly suppresses the TLR9-mediated human B cell functions during inflammatory processes. Based on our results, we believe that hydroxychloroquine can be beneficial in the treatment of B cell-mediated autoimmune diseases.
DOI: 10.1016/j.clim.2018.07.003
In a sense, HCQ is “anti-inflammatory”. Costedoat-Chalumeau and colleagues argue that TLR7 and TLR9 blocking is how HCQ helps lupus patients (see DOI:10.1016/j.lpm.2014.03.007).
Animal models of autoimmune disease
Multiple sclerosis
At high doses that are unsafe in humans, HCQ can reduce the severity of experimental autoimmune encephalitis (EAE), which is the closest thing to multiple sclerosis in humans. Redirecting At even higher doses and when used before onset of disease, it prevented EAE. However, that’s not very useful because chronic illness patients can only take a treatment well after onset of their chronic illness and the HCQ doses used were dangerous for humans.
Brown and colleagues also looked at EAE, though their human trial is more useful. They studied the combination of HCQ and Indapamide.
Faissner and colleagues studied the combination of minocycline and HCQ for EAE. https://doi.org/10.1177/1352458517728811
Autoimmune hepatitis
Uveitis (eye inflammation)
HCQ alleviates EAU by regulating the Teff/Treg balance and ameliorating RVECs dysfunction via the LOX-1/NF-κB axis. HCQ may be a promising therapeutic candidate for uveitis.
Frontiers | Hydroxychloroquine Alleviates EAU by Inhibiting Uveitogenic T Cells and Ameliorating Retinal Vascular Endothelial Cells Dysfunction
Risk
Some people do report negative effects from HCQ. Risk-wise, it is roughly in the middle of the pack- worse than ivermectin and most supplements.
It seems to be riskier in chronic illness patients than healthy people. (In healthy people, HCQ is regularly used as malaria prevention for those travelling to parts of Africa where malaria is an issue.)
The bottom line
Ever since COVID, HCQ has always been playing second fiddle to ivermectin. It did not win a Nobel prize like ivermectin or artemisinin.
As far as chronic illness goes, its popularity has certainly lagged ivermectin so the data on it is less reliable. It also seems to be a little riskier than ivermectin. In healthy individuals, ivermectin is safer. At the end of the day, you should probably consider ivermectin first before moving onto HCQ. It did help 1 person recover so there is certainly data to support its use for chronic illness.