First off, thank you to the 1456 or so of you who contributed your data! ![]() Your contributions helped put together a dataset on what people have tried, what the recovered reported as working, etc.
Your contributions helped put together a dataset on what people have tried, what the recovered reported as working, etc.
Highlights:
- Almost everything has been tried. If people are discussing a treatment on social media, there are probably many people who tried that treatment. You don’t need to do crazy experimentation because somebody else has (or will) put their body on the line for you.
- I’ve compiled a list of almost 110 treatments that were reported as helping the most. It is possible that these treatments are effective (though it is not proven that they are). You may want to avoid treatments not on the list as there is very little evidence to support their use (if the goal is recovery rather than symptom relief).
Other highlights:
- Some hyped treatments like IVIG, stellate ganglion block, etc. don’t appear to be that promising.
- The response rates are very low. The implication of this is that you will need to plan on trying many, many treatments if you are hellbent on recovery. (*Note: it is unclear if we have found any effective treatments. A survey can’t determine that.)
- Around a fifth of the recovered did not attribute their recovery to any treatment. If you simply do nothing, you may recover.
The data fleshes out what to expect and what a recovery plan might look like (assuming that we have identified effective treatments).
Treatments with plausible effectiveness
The survey asked:
What was the one treatment (or combination of treatments) that helped you the most?
I’ve compiled a list of every treatment mentioned in the answers (among those who recovered). Some people listed multiple treatments in their answer so there are almost 110 treatments listed for the 87 recoveries. See sheet #5 in this spreadsheet.
If a treatment isn’t on that list, you can simply let other patients be the guinea pigs. History suggests that there will be enough people who try crazy things given how many chronic illness patients there are out there (e.g. Facebook and Reddit support groups for Long COVID often have tens of thousands of members).
To see if a treatment is actually on that list, check for alternate names. I didn’t include alternate names like the marketing name of a drug, generic name, etc. To find some alternate names, see the guide to using the PES survey’s data dump. The data dumps also have information on a treatment’s popularity. Some treatments appear on the list simply because they were popular; it could turn out that they are worse than randomly trying a treatment (more on that later).
I’ve included brief (but incomplete) notes on treatment safety and RCT data. In some cases, RCT data strongly suggests that a treatment doesn’t work; in those cases you should ignore the survey data, which is less reliable. I would be cautious about ‘positive’ RCT data because the people behind the RCT may be dishonest, manipulating results, etc. It is not uncommon for researchers to report the opposite of what their data found.
Because survey data is far less reliable than you might expect, I recommend against trying anything risky based on survey data.
‘Recovery stories’ embedded in the survey data
See sheet #4 in the spreadsheet for raw-ish answers to the “what helped the most?” question, which can be seen as ‘recovery stories’. The first 10 rows look like this:
| Chronic illness | Paraphrased answer to What was the one treatment (or combination of treatments) that helped you the most? |
|---|---|
| Long COVID | Time |
| Long COVID | Time |
| Long COVID | Time. Avoid alcohol and caffeine. Eat low carb. Light excercise. Advil for flare ups. My long lasting condition is pericarditis. |
| Long COVID | Time, fasting, ivermectin, black seed oil, honey, probiotics, vitamin D, copper, raw camel milk, colostrum, light exercise, massage therapy, magnesium, sunlight, de-stress, antiinflammatory diet |
| Long COVID | Time |
| Long COVID | Time and rest |
| Long COVID | Rest |
| Long COVID | Exercise and time |
| Long COVID | No answer |
| Long COVID | No answer |
Summary of the ‘recovery stories’ / free-form answers
Treatments that helped the most were all over the place, even after I manually grouped the responses into general categories.
Multiple approaches = somebody discussing multiple treatments when they answered the question.
Full data available in sheet #3 here.
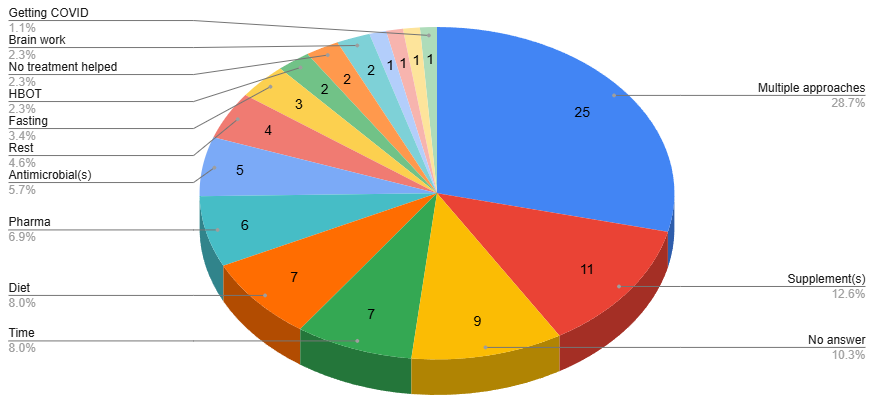
The combination of
- No answer
- No treatment helped
- Time
is arguably the most common answer.
The cause of Long COVID (and other chronic illnesses)?
Many popular theories about the cause (and therefore treatment) of Long COVID are represented, even though it is unlikely that multiple conflicting theories are all true.
- Persistent microbes → Antimicrobials, HBOT
- SARS-CoV-2 persistence → Paxlovid, antimicrobials, ?ivermectin?
- Cytokines → Maraviroc, statins
- Microclots → Triple therapy/anticoag
- Mind-body → Brain work/retraining, exercise
- etc.
What worked, but adjusted for how many times a treatment was tried
Another way of analyzing the data is to look at the intersection of people who recovered AND treatments that were rated highly. This will compensate for a treatment appearing frequently simply because a lot of people tried it.
The red line is what you could get from surveyees randomly picking answers. Any of the blue dots that appear above the red line may be better than random. You can search the full data in sheets #1 and #2 here.
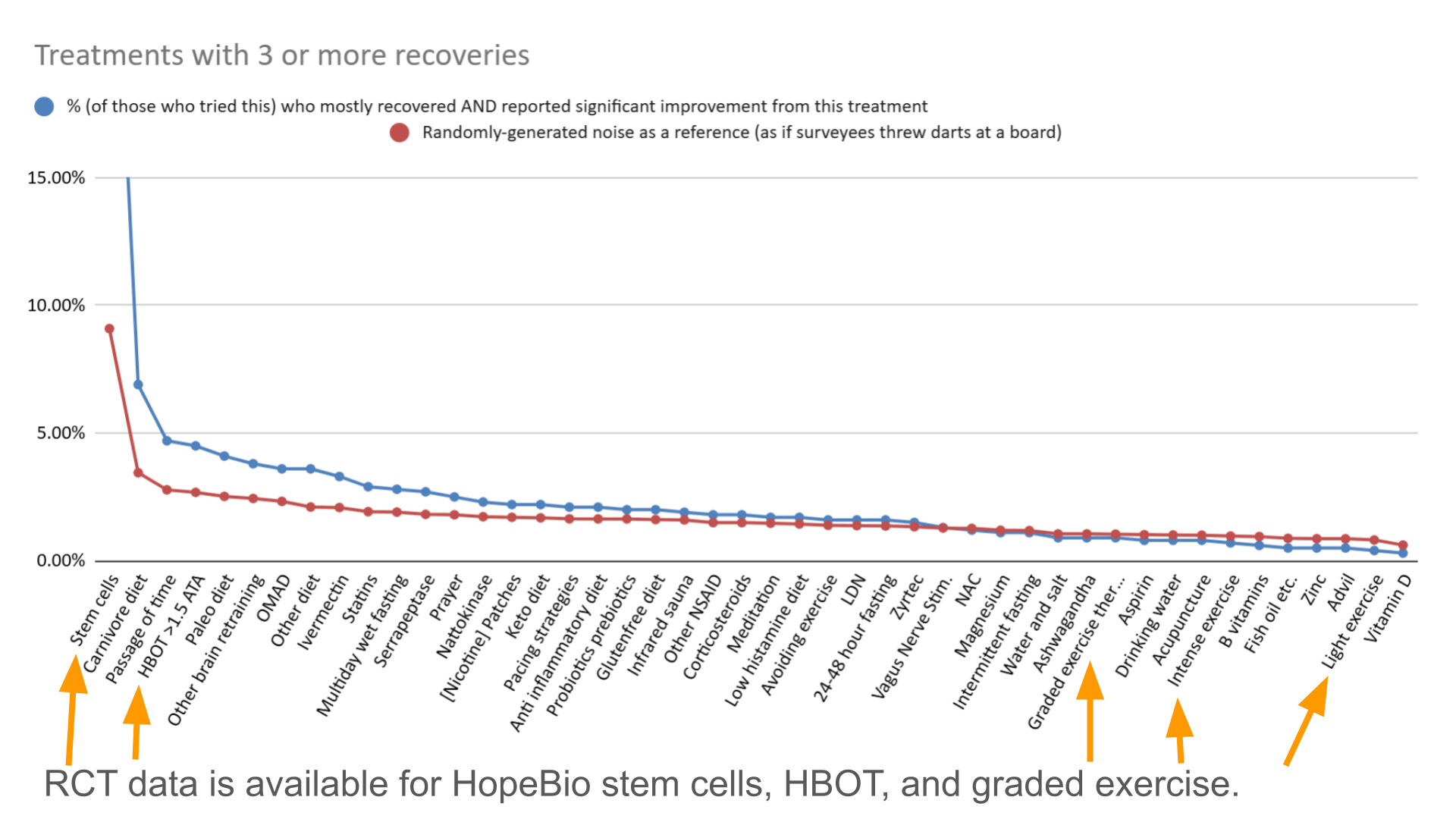
The #1 treatment in this chart, stem cells, is a mirage. Of the 3 people who reported significant improvement:
- One of them likely didn’t do stem cells at all. (For privacy reasons I can’t say why. However, researchers can sometimes figure out the identities of surveyees based on time of submission and/or the content of free-form responses.)
- One of them did Hope Biosciences stem cells, which failed their clinical trial.
So, please don’t do anything risky based on survey data- there are survey research limitations that cannot be overcome.
#3 is not a real treatment. I simply asked all participants about the passage of time. Somehow it outperforms almost everything else (!). We can infer that treatment response rates are, at best, very low.
Is exercise a mirage?
Exercise also has RCT data available (e.g. PACE for ME/CFS and other RCTs for Long COVID), though I believe that the available ‘research’ is highly questionable. The survey data suggests that interventions related to exercising less (avoiding exercise, pacing strategies) outperform the exercise-related interventions. Exercise also seems to underperform randomly selecting a treatment.
Patients frequently report negative experiences with exercise. It may cause more harm than good.
Brain retraining??
It appears to outperform, but that could be an artifact of survey design.
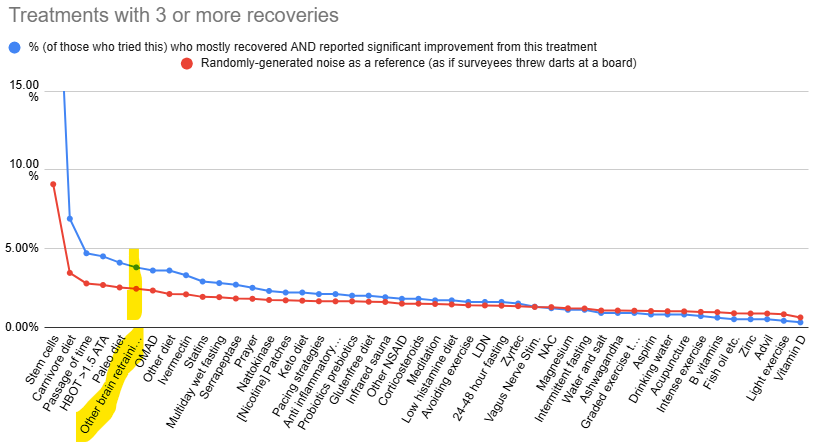
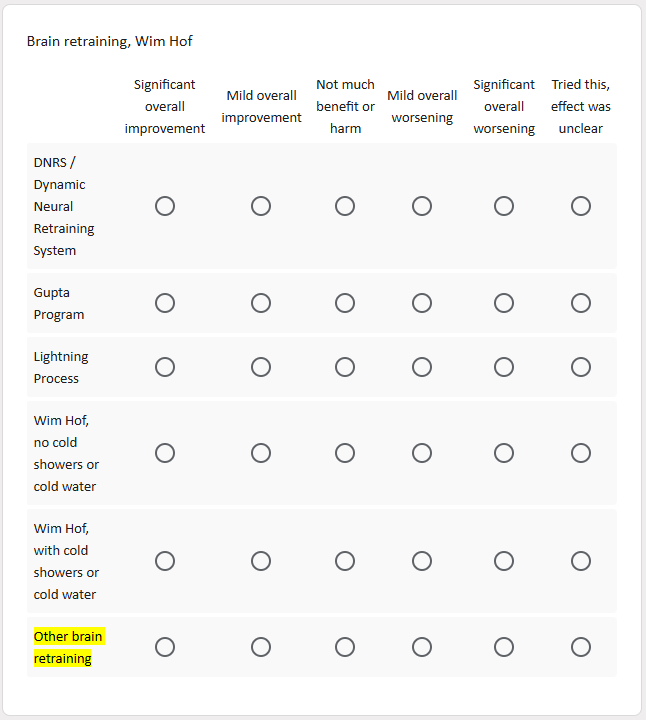
‘Other brain retraining’ refers to brain retraining other than DNRS, Gupta, and Lightning Process. (It’s not clear what type of brain retraining they did, though some people mentioned Sarno in the free-form responses.)
Suppose that surveyees tried multiple brain retraining methods. They might simply report results for the most successful of those methods. This would make it seem better than it is.
Also note that brain retraining was sliced up into sub-categories. This increases the chance that a sub-category will outperform- with 4 brain retraining choices instead of 1, there are 4 ‘shots on goal’ instead of 1.
The whole truth
Social media platforms prioritize engaging content over accurate content. For the fuller, more nuanced truth:
- Some data on the difference between engaging and accurate, e.g. 7.2K versus 1.9K views.
- What chronic illness researchers won’t tell you
- See the limitations section (and methodology notes) at the end of this post.
Closing thoughts
The current reality is that patients are trying treatments with very little evidence to guide their medical care. Survey data is helpful, but we have to be mindful about its limitations.
The survey data is useful for separating treatments with plausible efficacy and ones with questionable efficacy. While it appears that the survey data identifies promising treatments, the Long COVID RCTs for Hope Biosciences stem cells and Paxlovid have failed. Therefore, they likely cause more harm than good as the treatments have known problems and the RCTs weren’t able to find a benefit. HBOT on the other hand has mixed results. Overall, this suggests that many treatments won’t live up to their promise. So, it’s not a good idea to do anything risky based on survey data (or social media hype).
At the end of the day, we need more research to uncover the cause of chronic illness. Then, we can make meaningful progress on getting recovery rates up.
Methodology notes
Strengths of this dataset
While there are recovery stories on Reddit (see this summary and here) and Youtube, some of these stories seem to have people who are not recovered. This is because people define recovered differently- somebody who can’t work may still see themselves as recovered. (People define things differently.)
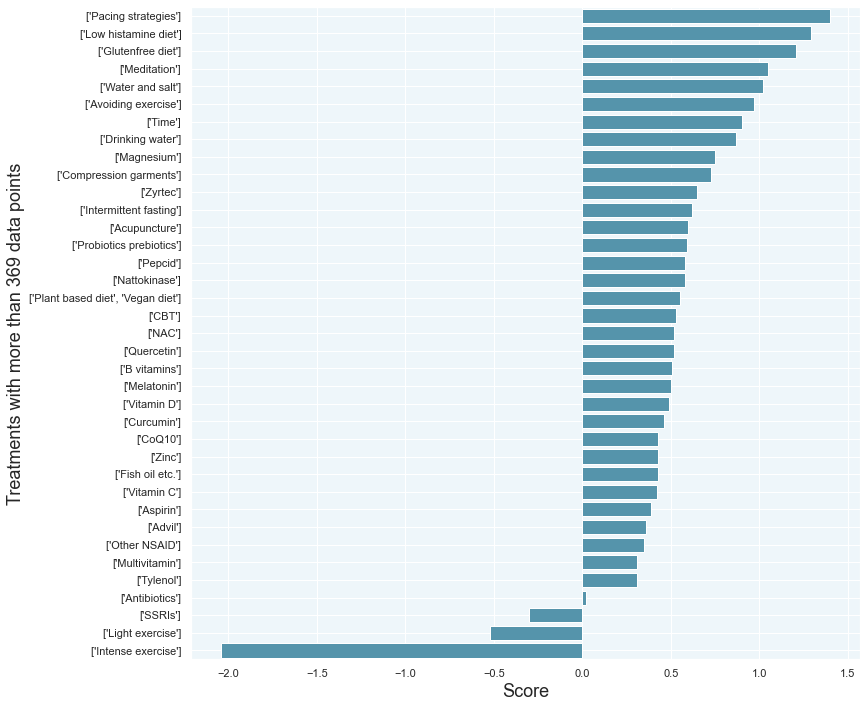
The non-recovered tend to report outcomes differently, causing certain treatments to be rated higher than they otherwise would be: prayer, low histamine diet, meditation, etc.
Freeform answers
This survey had both freeform and non-freeform answers. Freeform answers allow participants to name treatments not on the survey. Because of this, we can see that the majority of ‘successful’ treatments were among the 235 treatments surveyed.
The freeform question also focuses the answers onto the treatments that helped the most. This reduces the ‘spam’ from people saying that a long list of supplements helped.
Minimal bias against things that should “not” work
The survey included ‘janky’ treatments such as prayer (not shown below), meditation, gluten-free diet, drinking water before getting up in the morning*, etc. Unless we look at only recovered patients, those treatments score among the top.
LongHaulWiki.com/pes/2026-02-16-PES-analysis.html
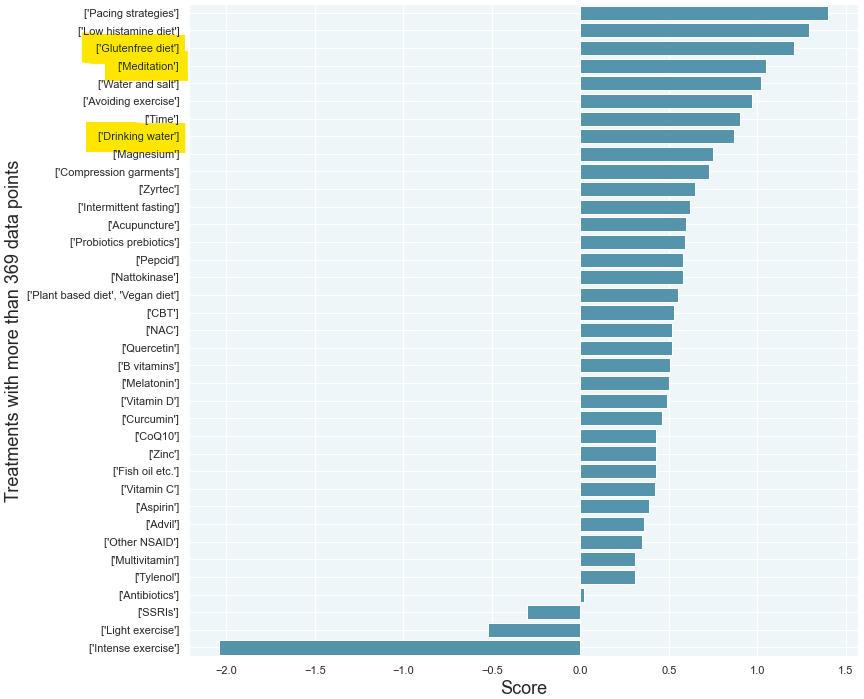
By including things that maybe shouldn’t work (and things the survey designer doesn’t take seriously), we can get a better picture as to how patients report their treatment outcomes.
*While drinking water is a recommendation for the treatment of POTS, not everyone who answered the question had POTS.
Where to find the full methodology
The full methodology of the survey is described in the video and slides here.
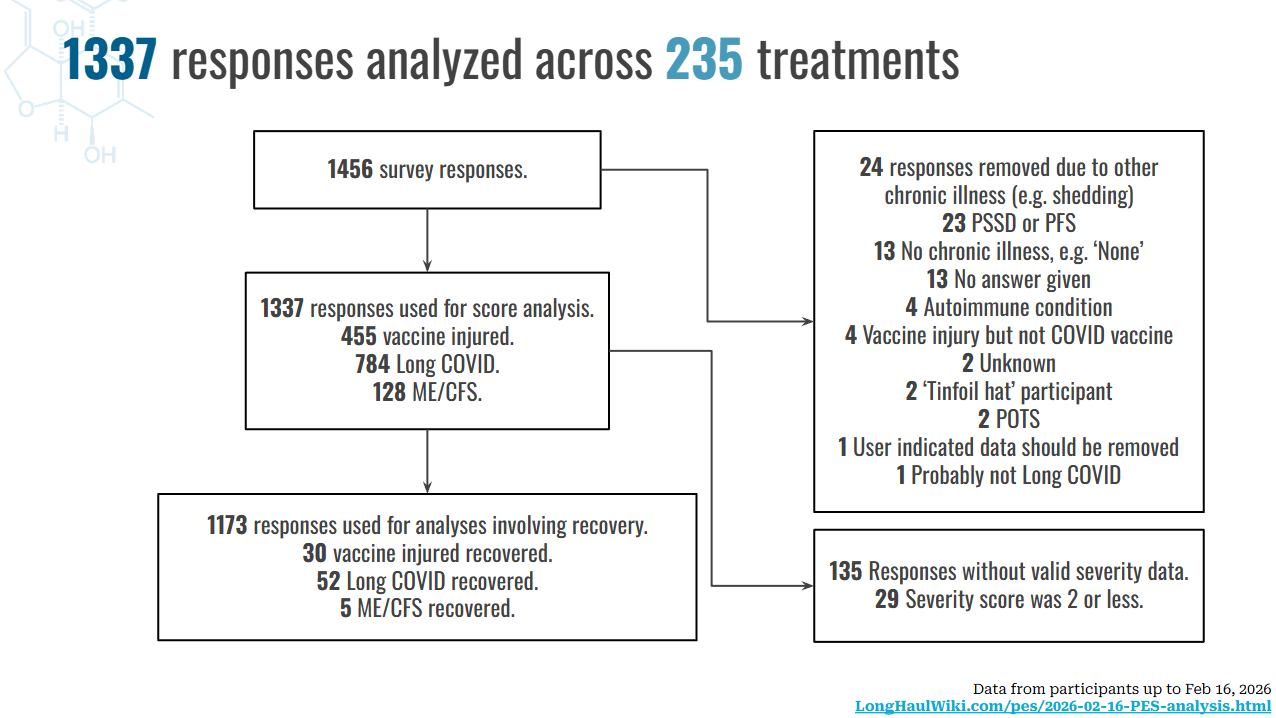
The flowchart for the Feb 16, 2026 dataset is as follows:
Limitations
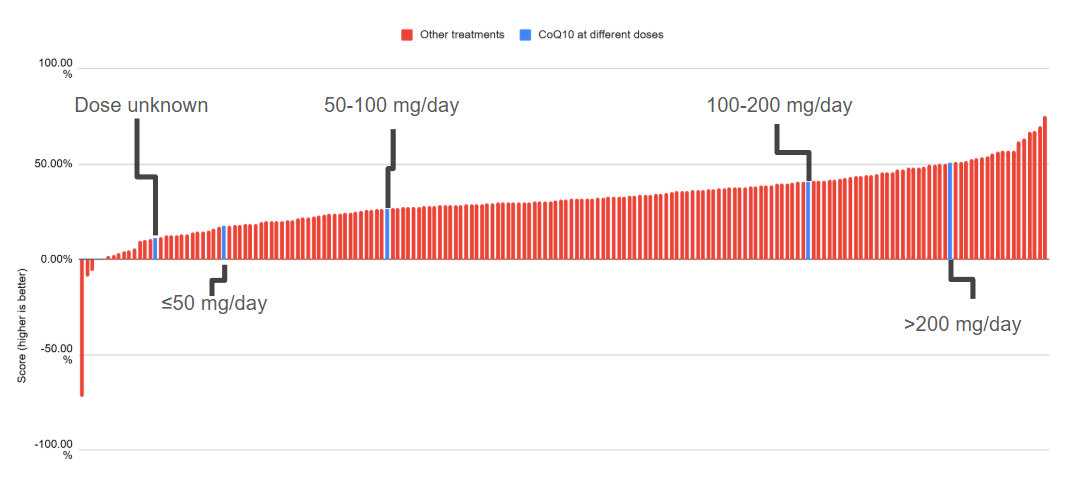
When chronic illness surveys measure treatment outcomes, they seem to mainly measure things unrelated to health outcomes. For example, in the TREATME survey data, an unknown dose of CoQ10 somehow falls outside the range of every other possible dose.
A deeper dive on what surveys measure is available here.
Some people answer surveys differently than other people. Some people have a ‘everything works’ style. Others say that nothing worked (except for prayer).
The truth about survey research
Because I don’t have a financial conflict of interest and I don’t grift, I can just say things that other researchers won’t say.
Many (or all) patients don’t know how they recovered. We can see this clearly with the survey data on Hope Biosciences stem cells, which failed its RCT. It turns out that one survey participant likely had erroneous beliefs about HopeBio stem cells helping the most.
If the patients don’t know what helped, then it’s clear that surveys can’t measure positive health outcomes. Surveys measure other things, like the logical connections that patients draw in their minds. Some patients will constantly tinker with how they do a treatment, e.g. by changing their dosage up and down. Eventually their tinkering will coincide with their health fluctuating in a positive direction. This may be why a few people report that everything that they tried works. There’s a logic to what they’re reporting.
Implications for healthcare
If the patients don’t know what treatments are helping, then doctors should stop their medical experimentation. If patients are coming back to them and saying that something ‘helped’, then there will be more medical decisions based on information that isn’t true.
The survey data clearly shows a bias towards ‘everything is helpful’. If you randomly pick a treatment, it’s almost certainly the case that patients, on average, view that treatment favorably.
This would lead practitioners down a path where they can believe in any of the Long COVID theories out there. If doctors treat patients for viral persistence (e.g. Paxlovid), they will see some ‘success’. If they treat for cytokines (e.g. maraviroc), they will see some ‘success’. But in reality, it’s just dangerous medicine. When we think we know what we’re doing but we actually don’t… that’s when we really get into trouble. We’d be safer getting our medical advice from Dr. Dre, Dr. Seuss or Dr. Pepper.
But patients want to chase recovery instead of medical care that isn’t harming them. So it’s hard to help people understand how science and medicine actually works when the truth is bitter. Patients are constantly being scammed by researchers who will say anything to raise funds (and keep their job), doctors who chase fame and money, etc. But those people rise to the top because they tell patients what they want to hear. So, if you can, please fight this by upvoting messages that you don’t necessarily want to hear. Sick people deserve actual science and progress towards a cure. The bumps in the road may be unpleasant but we need to take those bumps to get to a cure. Thank you. ![]()