I recovered from chronic illness. I’d like to see other people recover too. However, that won’t happen if patients have the wrong idea about what really goes on in science and medicine. I do research on chronic illness and I’m appalled at the bad behaviour out there. Let’s start with people like Judy Mikovits.
Bad actors are everywhere- including alternative medicine
In the survey I ran (“PES”), ivermectin was used by 11.8% of LC patients and 13.5% of ME/CFS patients. This suggests that the medical freedom movement has had a significant impact on patients (i.e. through treatment protocols).
The issue I have with the medical freedom movement is this: bad actors from mainstream medicine found refuge there. Judy Mikovits was heavily criticized by her peers for intentionally fabricating data in her ME/CFS research paper on XMRV. (See the retraction and this article on the reused photo controversy.)
Mikovits’ retracted paper resulted in millions of research dollars being wasted on verification studies. Patients also wasted money on ‘XMRV tests’ and treatments for retroviruses. But Mikovits didn’t stop being herself. Mikovits became the star of Plandemic, which is a cringe documentary on the COVID pandemic. She exploited the medical freedom movement by telling people what they want to hear and pandering to their political views on COVID lockdowns.
Mikovits is not the only charlatan who found refuge in the medical freedom movement. There is another researcher who had his/her paper forcibly retracted- this time for misrepresenting data to arrive at the desired conclusion. Obviously, that is not how science should be done. However, unlike Judy Mikovits, the retraction did not end this individual’s influence on research or medical care. Because I don’t feel like being sued by this individual, I won’t name him/her. However, this individual would go on to publish treatment protocols for Long COVID, postvax (vaccine injury) and other conditions like cancer. The cancer protocol suggests fenbendazole as a treatment. Fenbendazole is not FDA approved for human use.
What’s scary is that many medical doctors haven’t looked deeply into why this individual’s research paper was retracted. They blindly accepted the counter-narrative from this individual and the enablers (MDs, journalists). What you should know is that medical doctors are easily scammed- and that should scare you. Many MDs think that these protocols are scientifically and medically justified when they are not- it’s just somebody making stuff up. If you check the referenced sources in said protocols, some of the references don’t even say what they’re supposed to say! In one of this individual’s treatment protocols, not all of the randomized controlled trials are actually randomized controlled trials. This individual never stopped his/her misrepresentation of ‘evidence’.
- Note: I’m not against the use of ivermectin for chronic illness. Ivermectin is simply a proxy for the medical freedom movement’s influence. Patients should be careful about the freedom movement exaggerating ivermectin’s safety and efficacy.
Researchers can fall behind if they don’t play the game
There are strong incentives to tell people what they want to hear. In 2015, Ian Lipkin said: “Three to Five Years* to Solve Chronic Fatigue Syndrome”. That obviously didn’t happen.
And then in 2025:
“There’s so much hope right now. We can finally get somewhere with this.”
(Source: Health Rising)
The issue is that researchers get fired if they aren’t bringing in enough research funding. So, they tell patients what they want to hear because it helps them bring in research money. Capitalism weeds out the researchers who don’t want to play this game. This affects chronic illness journalism too- hope porn is a formula that works. I don’t blame Cort Johnson for echoing Ron Davis’ optimism in 2015:
That sounds really fast, but Lipkin’s time-frame is not that far off from Ronald Davis’s 5-10 year time-frame (provided he gets the resources as well.) (or Dr. Montoya’s).These eminent researchers believe that given the technology present today we could understand ME/CFS fairly quickly - if enough resources were brought to bear.
Limitations of survey research
I’ve done survey research on chronic illness. And here’s the dirty secret: surveys measure a lot of things unrelated to health outcomes. I wish that wasn’t the case. I wish that chronic illness was easier to figure out. However, we need to recognize that survey research has very serious limitations.
For example, the survey run by Martha Eckey (LongCovidPharmD) was published with a ‘top 20’ list that includes co-enzyme Q10. The problem is that co-enzyme Q10 is simultaneously among the best and worst treatments. As the survey asked about CoQ10 at different dose ranges, some doses were among the bottom and others were among the top.
The chart plots score on the y-axis. Higher is better. CoQ10 treatments are in blue. Score is defined in the top 20 list below.
The data is available on Martha Eckey’s substack and in the paper published by Eckey and colleagues. I took the data and reworked it into the chart above.
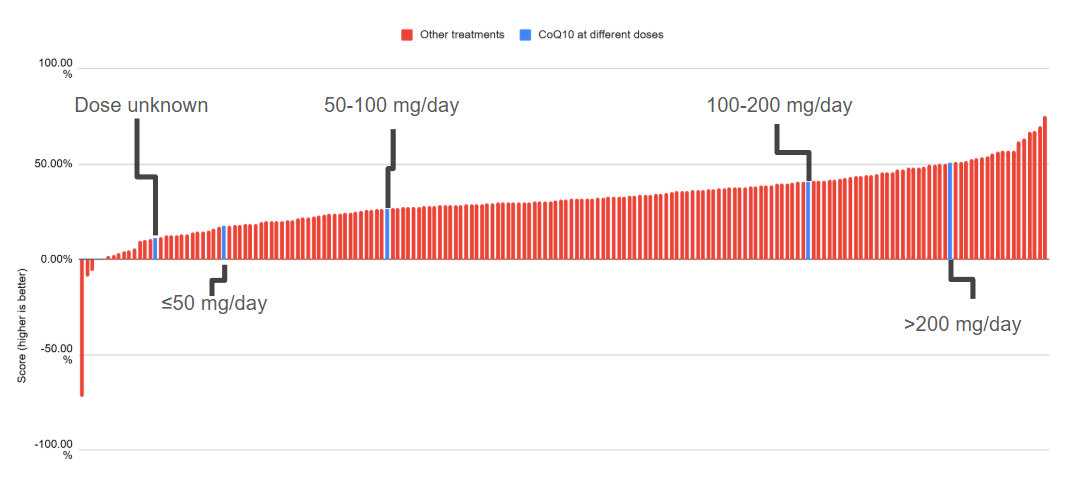
CoQ10 is in the top 20 list. Available on Eckey’s substack and as Figure 2 in the published paper. Click to enlarge. Eckey collected data on LC, MECFS, and postvax. The published paper omits postvax data (it seems that they collected very little so the omission simplifies their analysis by a lot).
We would expect that the dose unknown results to fall somewhere between the other dosages. It does not (!). The results should not be medically possible. The survey is almost certainly measuring things unrelated to health outcomes.
Think of it this way. Suppose that beneficial treatment effects are extremely weak (on average). There would not be much signal to measure. So what will happen is that the treatment effect will make up only a tiny portion of what gets measured. Or suppose that many patients simply don’t know what helped. Then surveys are asking questions that the surveyees can only inaccurately answer. If only some patients don’t know what helped, it can be enough to screw up the data.
- Side note: When I read the survey, I got the impression that Martha Eckey was in really bad shape when she made it.
 There are inconsistencies in the wording, one treatment section can be skipped but others can’t, etc. That’s why I don’t blame her for not digging extensively into the data she collected. I’m very impressed by how much she got done despite suffering from Long COVID.
There are inconsistencies in the wording, one treatment section can be skipped but others can’t, etc. That’s why I don’t blame her for not digging extensively into the data she collected. I’m very impressed by how much she got done despite suffering from Long COVID.
Patients have different ideas about what treatments actually are
What are ‘pacing strategies’? On Raelan Agle’s Youtube channel, you can see her describing ‘pacing’ as a tool for enabling more exercise. This may or may not be related to her positive attitude towards brain retraining; brain retraining often involves the view that mental blocks are holding patients back. Her version of pacing involves the gradual re-introduction and increase of exercise into the patient’s life rather than a decrease of exercise.
There are large communities of ME/CFS patients (and advocacy organizations) who have strong views about exercise being harmful. However, not all patients share these views. A few ME/CFS patients in survey data do report positive experiences with Graded Exercise Therapy (*that doesn’t necessarily mean that GET helped them). So, it’s possible that a small number of survey participants viewed pacing as an increase in exercise- completely different to what other patients are doing.
The point is this: communicating with patients is really hard. Miscommunication and misinterpretation is easy because people have different ideas about what words mean.
While invisible illnesses are often diagnosed based on patient-reported symptoms, that reporting is prone to miscommunication. The PLRC group reported that the prevalence of diarrhea in Long COVID was 59.7%; Kenny et al. report 2.6%. If you read the PLRC survey, it’s easy to see that the issue is likely due to survey design. Everybody gets diarrhea every once in a while; that likely accounts for most of what the PLRC survey measured. Presumably they wanted to measure medically unusual diarrhea but that is not what their survey actually measured.
Pro-exercise RCTs like the PACE trial won’t go away anytime soon
Exercise is a statistical outlier on surveys as they massively underperform everything else. However, some patients do report positive experiences with exercise, graded exercise therapy, etc. One analysis of social media recovery stories found that 51/60 stories mentioned some form of exercise; ChatGPT hallucinations do not explain the high prevalence (I spot checked the results).
From the clinician’s perspective, the clinician may have a justifiable basis to believe that exercise is a good idea (even though it probably isn’t). The people who had very negative experiences with exercise (e.g. Jennifer Brea) have a higher chance of avoiding the pro-exercise clinicians. So, the clinicians will interact more with the exercise believers. When randomized controlled trials enroll patients, it is likely that the trial will enroll a lot of pro-exercise people.
The clinicians may also harbour selective distrust of patients. For example, Survivor Corps founder Diana Berrent (Diana Guthe) said that she had Long COVID. Currently she says that she doesn’t. Clinicians may have understandable reasons to distrust people with chronic illness. This can lead to selective filtering of patient-reported information, which can enable the belief that graded exercise therapy is a good idea.
After the data is collected, there is an incentive to manipulate the data to arrive at sexy results. Many journals aren’t interested in publishing null findings (i.e. that exercise doesn’t help).
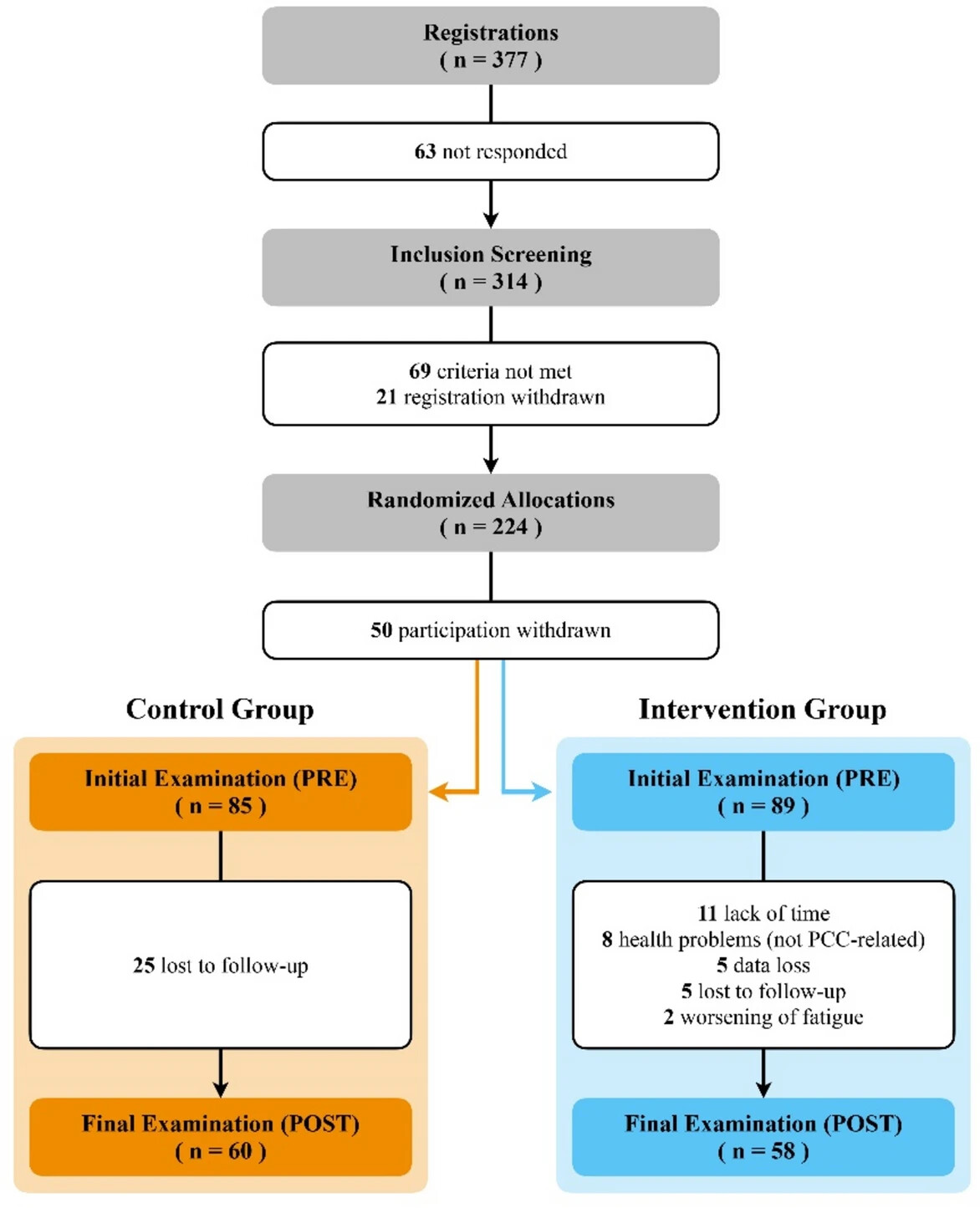
One common way of playing statistical games is to change the primary endpoint. Basically moving the goalposts around. Another way is to selectively eliminate unwanted data. In a study which found a benefit to their ‘symptom-titrated exercise program’, the study eliminated data from participants due to worsening of fatigue (2), health problems not PCC-related (8), and data loss (5). Now this doesn’t mean that these researchers intentionally manipulated their data. However, other researchers could selectively choose how they clean up their data to arrive at sexy-sounding results.
Note: It is not clear to me how the intervention group had 8 people with health problems (not PCC-related) while the control group had 0. I haven’t asked the authors about this coincidence.
Effects of a symptom-titrated exercise program on fatigue and quality of life in people with post-COVID condition – a randomized controlled trial | Scientific Reports
Also, researchers can do bad faith data clean-up in a way that’s very hard to detect. For example, suppose that a patient accidentally gets the intervention instead of the placebo. The researcher should remove that patient from the placebo group because they obviously didn’t get the placebo. But if they don’t do that, then how would you know???
The danger of clinical experience
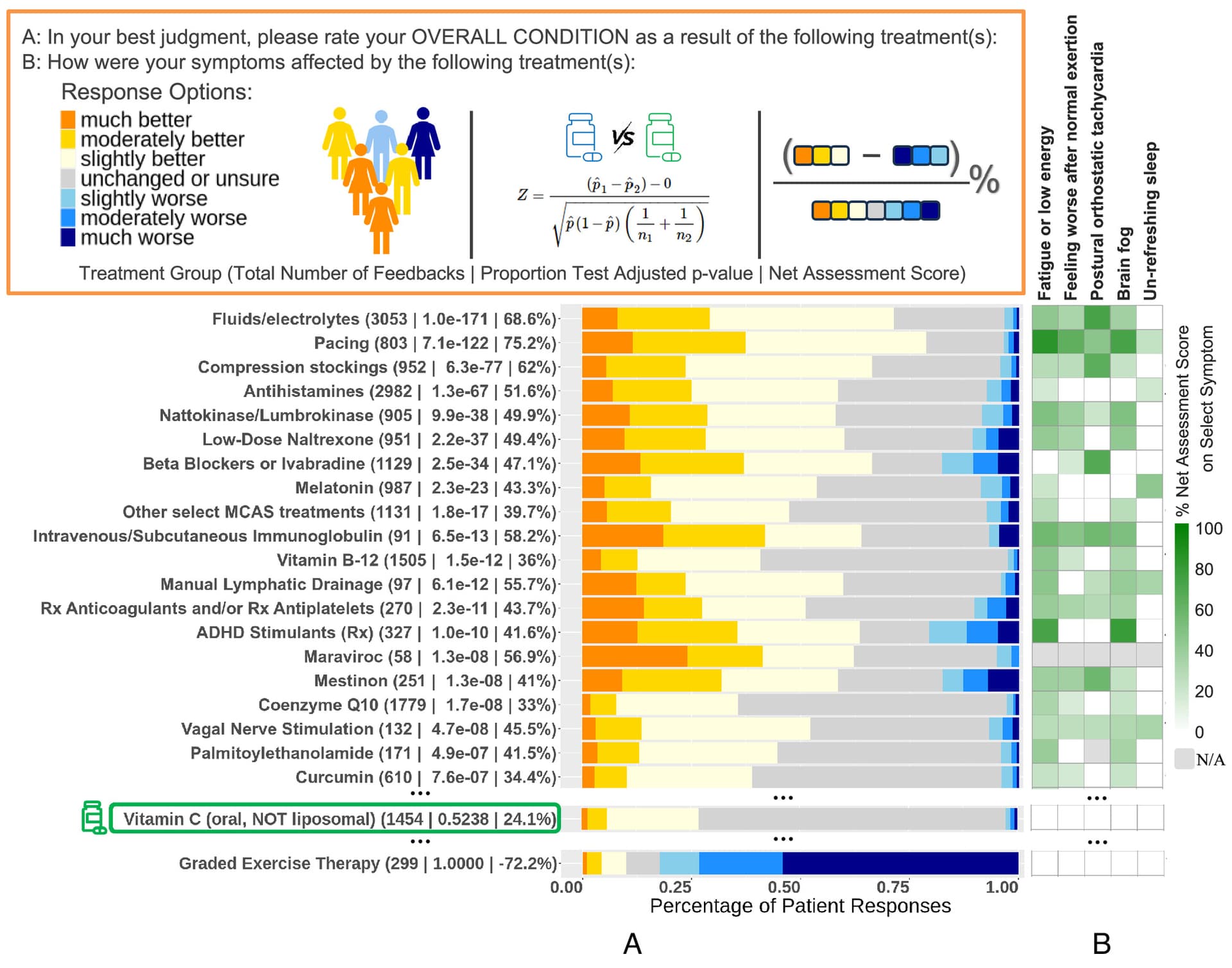
Patient-reported experiences (as measured by surveys) are quite different than what the randomized controlled trials on Long COVID are finding. For the most part, the RCTs have not been meeting their original primary endpoints. Therefore it is likely that most of the treatments studied in RCTs don’t work. In surveys however, patients (on average) are reporting positive experiences with almost every treatment. Unlike the RCTs, everything works…
The same chart as earlier. Some treatments are represented by multiple bars because the survey asked about dosage. Other treatments have been merged together (by Eckey et al. when they published their supplementary data).
- Please note that survey participants behave differently than each other. Some will consistently report no benefit. Others will report that (almost) everything works- see slide 10 here for an analysis of survey data I collected.
If some patients get it wrong, then how can clinicians get it right? I would argue that doctors simply can’t get it right. Currently, the problems are too difficult. Gathering accurate, reliable data is incredibly hard and we haven’t solved those problems. On a practical level, clinicians could focus on harm avoidance; high-risk treatments should be difficult to justify.
I do understand that Dr. John Chia has published his experiences on using remdesivir in ME/CFS patients. Unfortunately, a different study describes 1-3 deaths caused by remdesivir (remdesivir on acute COVID patients; unblinded RCT). Some people I know started using remdesivir’s metabolite (‘GS-44’) after they saw what Chia was trying. I am concerned that well-intentioned experimentation will eventually end in disaster. Jenny Rowbury learned this the hard way.
Our future selves will look back on this era and consider the medical practices to be misguided and ill-informed.
Reddit users reveal how unscientific their field is
Redditors at r/medicine have this to say:
Clinical practice isn’t really evidence based, a lot of things we do mostly because it’s the way it’s always been done. There is so much we don’t know about medicine and most of the time we are taking educated guesses. Most diagnosis and treatment plans are a risk/ benefit analysis of probabilities with a significant (more than 5%) error rate. We are just not that good at medicine yet.
There is a large discrepancy in the publics expectation of how accurate we are and the reality. I think in 100 years we will look back at the barbaric way we practice medicine currently even in our best institutions.
angrywaffles_ MD
People subscribe to evidence based medicine… until they don’t.
Basically just justifying what they like to do or believe it by using EBM but will conveniently ignore evidence when it suits them.
kungfuenglish MD
There are also threads about Long COVID not being real. ![]()
Is “Long-Hauler” the new “CFS/ME/Fibro/Chronic Lyme”?
SPFMN MD
A new study finds that most ‘Long COVID’ symptoms are not independently associated with evidence of prior SARS-CoV-2 infection (except loss of sense of smell), but is associated with belief in having had COVID.
modest811 medical student
Reddit users also discuss p-hacking to manipulate data to get the desired results and the dirty secrets of academia.
Bad science and bad medicine get in the way of recovery
Some people do recover from chronic illness. But patients won’t get there if they are scammed by all of the unreliable or fabricated information out there. Patients don’t have to waste money on unsound science like XMRV tests. Accuracy is the way forward.