
- COVID vaccines seem to cause more harm than good in chronic illness patients.
- Ivermectin is a reasonable treatment for Long COVID.
- Research money is being wasted on the microclots theory.
COVID vaccines and vaccinations in chronic illness patients
Let’s start with the most controversial and politicized topic. Now that a good body of evidence exists, it is clear that most studies are showing that vaccination causes more harm than good in chronic illness patients.
I’ve put up a 8 and a half minute video along with its slides:
6 out of 8 relevant studies indicate a net harm. 2 of the studies are higher quality as they are prospective observational studies rather than (retrospective) surveys. Both of the higher-quality studies indicate a net harm*. (*To be fair, one of the studies examined the effect of vaccinations on patients who had already been hurt by them and its results were not surprising.)
One particularly troubling anecdote is Heidi Ferrer, whose Long COVID symptoms exploded after her Moderna vaccination. Her eulogy (https://web.archive.org/web/20220309031441/https://girltomom.com/a-prayer/heidis-eulogy) provides some details on her health post-vaccination. Moderna set off a chain of events that led to her trying Ambien for crippling sleep issues post-vax and a poorly-executed suicide. It is not clear what factors played a role in her death (Ambien, Long COVID, vaccination side effects, her controlling husband, etc.); suicide is a known side effect of Ambien/zolpidem. However, the chain of events likely would not have occurred if she had not gotten vaccinated.
While higher-quality evidence would be ideal, it does not look like we will get it. Yale conducted its Recovery study (NCT04895189) which studied the effect of COVID vaccination on unvaccinated Long COVID sufferers. It would have added another prospective observational study to the body of evidence. However, its release has been pushed back 2 years to 2025. We will have to base decisions on the current body of evidence.
This whole debacle certainly highlights problems with the current ecosystem of “advocacy” groups, clinicians, and researchers. Medical recommendations were given without strong evidence that vaccination was appropriate in chronic illness groups. After patient groups started surveying patients and finding evidence of harm (e.g. ANZMES, ME Association UK, etc.), they largely did not try to correct the record. Instead, they continued to recommend COVID vaccinations anyways.
Ivermectin is a reasonable treatment for Long COVID
Many (though not all) Long COVID support groups have censored discussions surrounding ivermectin when the molecule became associated with “anti-vaxxers”, Donald Trump / MAGA, conspiracy theories, etc.
The overarching issue is that current Long COVID treatments are not very good. On average, their effects are mild as many people do not respond to the treatment. Because of this, it is difficult to tell if a treatment helps as it takes large numbers of patients to detect weak efficacy signals.
Nonetheless, it turns out that ivermectin is one of the top treatments right now. It’s not a wonder drug and it doesn’t work for most people. But, it does happen to be one of the top drugs. Data and some safety information in the primer below:
Research money is being wasted on the microclots theory
Microclots are found in healthy people.
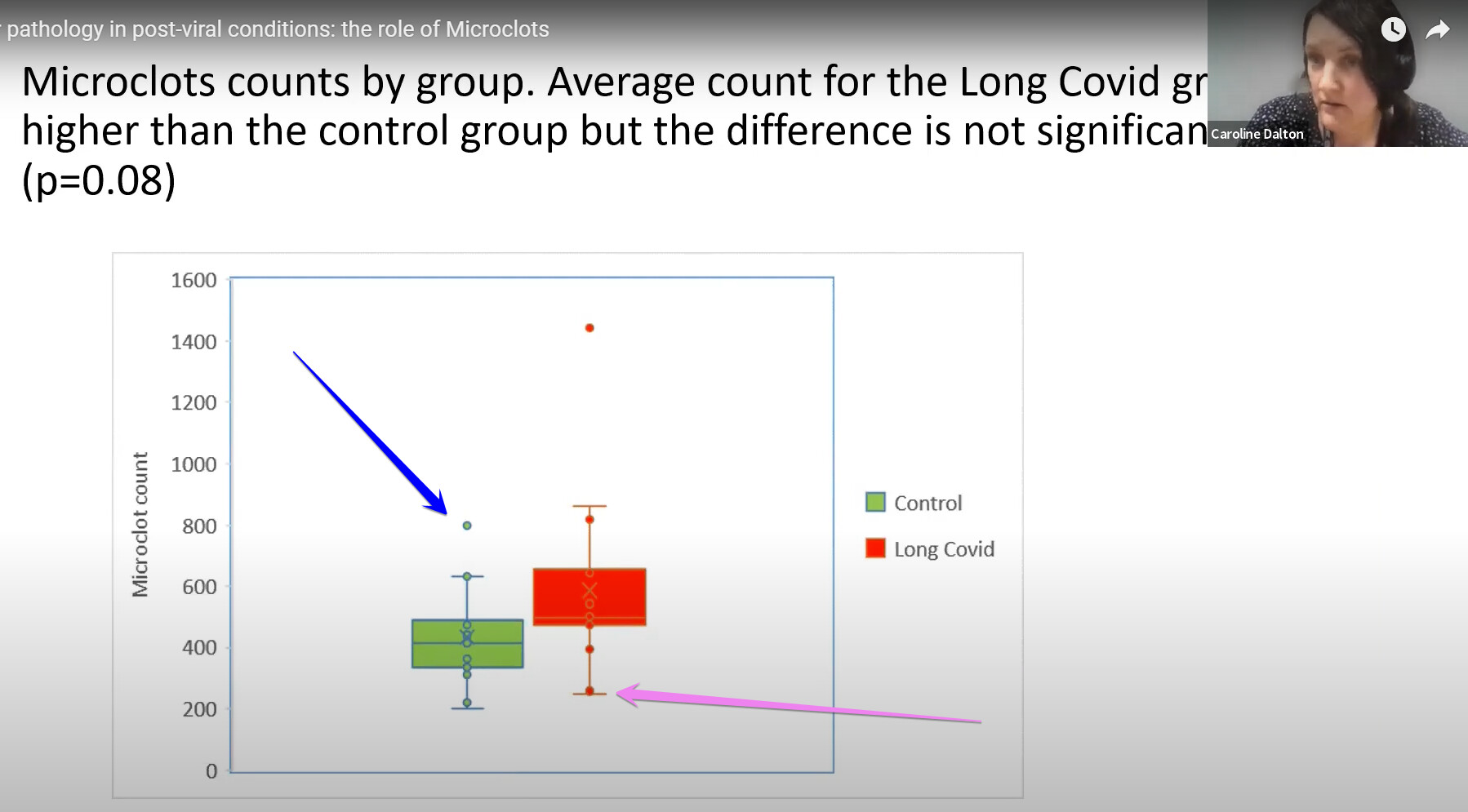
More specifically: abnormal levels of microclots are found in healthy people (uncommon), Type 2 Diabetes patients, Long COVID, acute COVID, and ME/CFS patients. You don’t have to take my word for it. Doug Kell discusses this on his website (live version, archive.org version). Caroline Dalton presented her data in a presentation with Resia Pretorius. According to her data, most Long COVID patients have the same level of microclotting as normal healthy controls.
“There’s quite a bit of overlap”
- Caroline Dalton
I’ve added blue and purple arrows to the diagram below to show the healthy control with the highest microclotting level and the Long COVID patient with the least microclotting.
I don’t want to get into the weeds too much here. For a deeper dive into what’s wrong with the science, see the post below and the post above it:
The big picture is that the emperor has no clothes. Back in 2022, LC and ME/CFS patients were trying triple anticoag and discovering that it is not a miracle cure. Chronic illness sufferers who work with #TeamClots, e.g. Asad Khan and Harriet Carroll, also realized that it wasn’t a miracle cure for their health problems (LC and vax injury respectively). The treatment failures show that the Pretorius et al. preprint (version 1) was likely misreporting patient outcomes when it claimed that all 24/24 patients ‘recovered’ on triple anticoag. The #TeamClots track record is 0/2 while their preprint dubiously claimed that their track record was 24/24.
Unfortunately, we’re still talking about microclots in 2023 and millions of dollars in research funding will be spent studying microclots. There was a lot of bad behaviour from people who pretended to know what they’re doing and bad behaviour from people who knew exactly what they were doing.
Putting patients first
In the battle of ideas, censorship is the admission of defeat.
Patients are going to discover the truth. What needs to happen is for more patients to shift to platforms and support groups where information doesn’t get censored. I can’t imagine this post surviving at r/CovidLongHaulers and certain other venues. And that’s a huge disservice to really sick people who should benefit from the free flow of ideas.
To solve that problem, there are certain groups that I will be trying to help grow (though I do not have a focus on Long COVID or ME/CFS):
- This forum at https://forum.sickandabandoned.com/
- *Reddit: r/VaxRecoveryGroup which is owned by Zelly.
- *Facebook: My Canadian vccn injury Facebook group
- *Facebook: Cat Parker’s Facebook group
- Trialsite (independent news): Cat Parker’s TrialSite News group
- *Certain Discords. See this list of support groups.
In the long run, the healthiest support group ecosystem would have good actors running them so that censorship issues don’t happen again. Secondly, spreading out ownership over at least 2/3 people would be ideal. This would avoid problems with power being concentrated in one support group owner who then decides to make controversial moderation decisions.
The free flow of ideas really matters because the cost of censorship is sometimes human life. There was a ME/CFS patient named Jack who became vaccine injured and started participating in the vax injury support groups. His vax injury likely played a role in his eventual suicide. This level of suffering could have been softened if patients had access to information that could have steered them away from questionable decisions.
At the end of the day, the true measure of our humanity lies in how we treat those who can do nothing for us.