Certain parties have released a treatment guide for Long COVID, which surprisingly suggests Paxlovid as a treatment for Long COVID. The guide cites two failed randomized controlled trials on Paxlovid for LC- this should have been enough to recommend against the use of Paxlovid rather than for it.
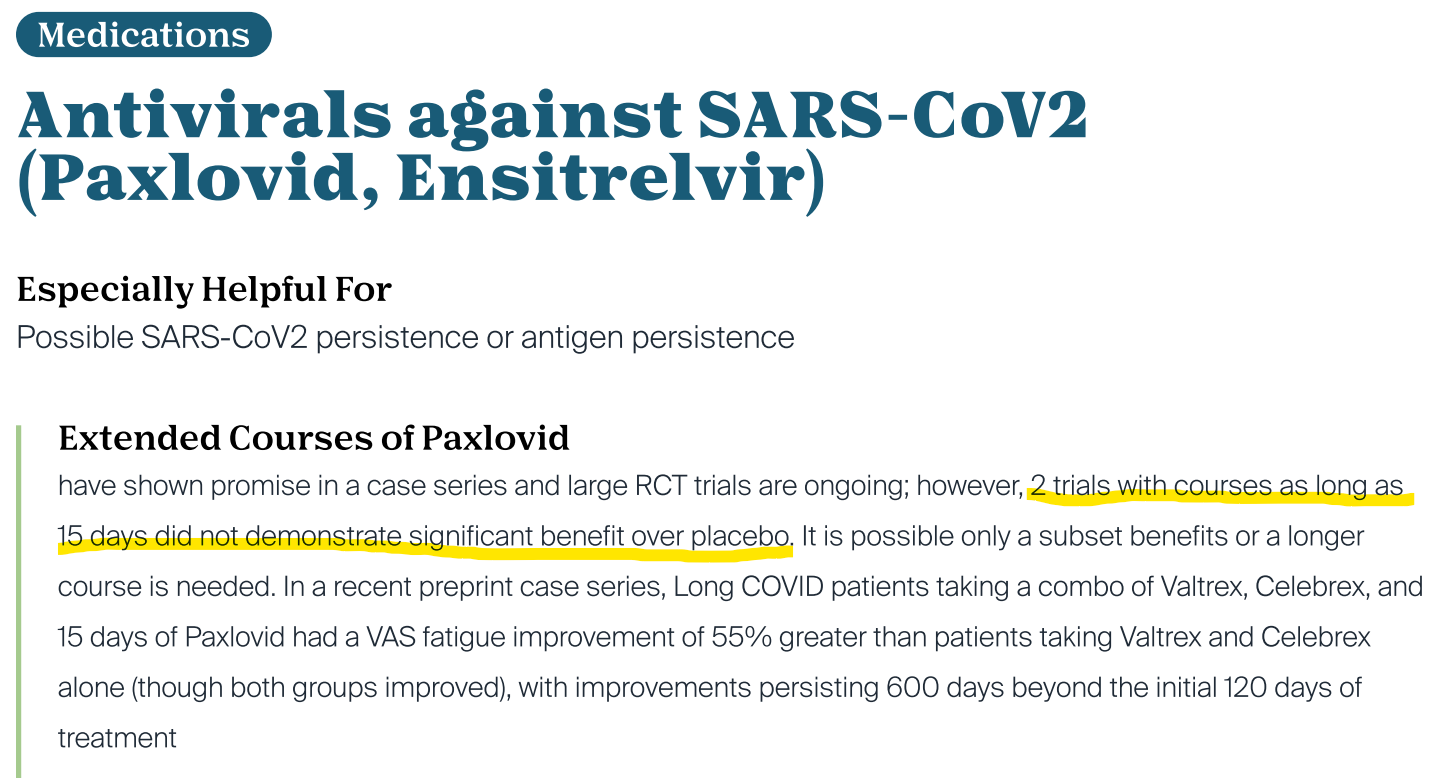
These trials failed because they did not meet their primary endpoints. The scientific evidence strongly suggests that there is no benefit to Paxlovid for Long COVID.
With no demonstrated efficacy and known safety issues (Paxlovid contains the HIV drug ritonavir), the current science suggests that Paxlovid for Long COVID will do more harm than good. The data points towards doing the opposite of what the guide suggests.
The bottom line
Many people have had their lives turned upside down by Long COVID. We should be trying to guide patients towards better health rather than away from it.
Patients can look out for each other by being more informed and raising awareness about bad science. In some cases like this one, bad science isn’t that hard to spot. I hope that all of you out there will eventually recover from chronic illness like I did. ![]()
Appendix- an explanation of clinical trials and how medicine should work
If you run a trial and measure lots of things and analyze it lots of ways, you will likely find something due to random luck.
- Measurements = walking tests, surveys, etc.
- Analysis = looking at subgroups like male versus female, old versus young, etc.
If you do that 20 times, then you will likely find something that happens 5% of the time or less. In other words, you will likely find a statistically significant result. “P-hacking” is when researchers intentionally do a lot of different analyses on the data to find a statistically significant result.
Pre-registering a trial is one way to prevent most forms of p-hacking. Before the trial starts, the researchers will state what the primary endpoint (or endpoints) will be. They pick what measurements and analyses they will use beforehand and they post that plan publicly (e.g. clinicaltrials.gov). This should prevent them from changing the goalposts after the fact, adding a layer of protection against erroneous findings.
If the primary endpoint is met, then the trial will likely be deemed a success. The opposite also applies. A failed trial adds significant evidence against a treatment. Unfortunately, the reality is that most papers will try to hide the primary endpoint if it isn’t met. That finding will be buried somewhere in the middle of the paper. It’s not immediately obvious that the trial has failed. However, if the findings do get published, then we can figure out what actually happened in a clinical trial.
Yes, technically, there is a chance that a future Paxlovid trial meets its primary endpoint
Yes, technically, randomized controlled on humans are rarely definitive. Maybe the study didn’t do a particular treatment right (dosage too low, treatment not long enough, etc.). Through sheer luck, a trial may meet its primary endpoint (e.g. you run 20 trials on the same drug). Through sheer luck, a mildly effective drug may fail a clinical trial (though the chances of this happening twice are very low). However, the current available evidence is already leaning against that treatment.
Paxlovid is unusual because it is well above average in terms of how much evidence is against it. However, this is because there aren’t a lot of Long COVID RCTs that have been completed.
Or we can look at it this way. If you have a hypothesis, find reliable evidence that goes against that hypothesis, and then simply ignore all of that evidence… that would be the opposite of data-driven medicine. If you promote treatments regardless of the data coming in, then it’s not data-driven!
Further reading
Long COVID research has a history of bad science. Here’s a guide on how to spot bad survey research, which will let you spot unreliable science and help you understand problems with the scientific literature.