Genome Wide Association Studies (GWAS) can find subtle influences of genes on a health condition. They map out important gene variations to see if any of them are unusually common or uncommon among a particular health condition.
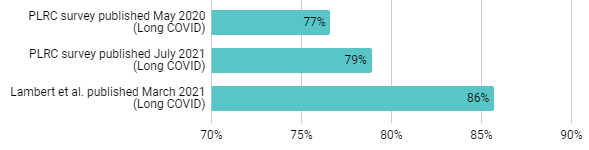
We already know that Long COVID is more common in people who are female.
Data compiled here: https://docs.google.com/spreadsheets/d/1bxzgvtOFBzvIQSnFiJqEQ7Lt7wzijpDwBcdnl87gw5I/edit#gid=2093830457
*The data above is from surveys which asked about gender rather than biological sex.
Unfortunately, a recent GWAS study by Lammi and colleagues (pooling data from multiple studies) found that only the FOXP4 gene has a strong connection Long COVID.
The study found that a particular genetic variation was associated with a 1.63X chance (odds ratio) of having Long COVID.
The C allele at rs9367106 was associated with an increased risk of Long COVID (OR = 1.63,
95% confidence interval (CI): 1.40-1.89, risk allele frequency = 4.2%).
That odds ratio of 1.63X was lower than the >3X odds ratio of being more likely to have Long COVID if you’re female. It’s not a very strong risk factor.
The researchers believe that “the connection between FOXP4 and Long COVID may be rooted in both lung function and immunology”. The gene is expressed in both alveolar cells and immune cells in the lung.
Long COVID may be almost entirely caused by the environment???
Unfortunately, the study doesn’t say a lot about what causes Long COVID. It does strongly suggest that your genes are fairly unimportant (other than male versus female).
EDS
This type of study would pick up on Ehlers Danlos Syndrome caused by genetics. However, it doesn’t seem to have found a signal there. I suspect that Long COVID patents are more hypermobile (flexible) than the general population. I don’t know if anybody has surveyed Long COVID patients to determine their Beighton score yet.
Hot take
The results are disappointing. Even in conditions that are acquired from the environment (e.g. EBV and Varicella Zoster Virus / shingles), GWAS studies will pick up some signals that can point to the underlying mechanism. That did not happen here.
There is evidence that Long COVID is connected to viral reactivations of EBV and VZV. However, this GWAS study didn’t find a signal for genes connected to those infections (for a list of those genes, see Table 1 in this review paper). Long COVID probably isn’t tied to a single underlying infection.